*Correspondence to: Dr. Katherine Brakora, Texas A&M Naresh K. Vashisht College of Medicine, Bryan, Texas, USA
Received: Jan 02, 2026; Accepted: Jan 17, 2026; Published: Feb 11, 2026
Citation: Brakora K (2026) Asymmetrical Bilateral Presentation of Palmaris Profundus: A Case Report. J Anatomical Variation and Clinical Case Report 3:12. DOI: https://doi.org/10.61309/javccr.1000
Copyright: ©2026 Sosale P. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ABSTRACT
The palmaris profundus (PP) muscle is a rare anatomical variant of the forearm musculature. It has a low prevalence and a wide range of presentations. Its proximity to the median nerve within the carpal tunnel stipulates its clinical significance with respect to both surgical and diagnostic contexts. During routine cadaveric dissection of a 97-year-old male, bilateral variants of the PP muscle were identified. The right forearm exhibited a Type I PP, originating from the anterior surface of the radius and inserting into the flexor retinaculum. The left forearm revealed a previously undocumented variant, originating from the proximal radius and coursing deep to the flexor digitorum superficialis, inserting into the palmar aponeurosis. This configuration does not align with existing classifications as is proposed as Type VI: palmaris profundus inversus radialis proximalis. This case study will contribute to the anatomic literature by expanding and bringing awareness to the various classifications of PP variants. Recognition of this anatomical abnormality is essential for anatomists, surgeons, and medical educators as they may influence outcomes in carpal tunnel release, tendon grafting, and peripheral nervous system assessments.
Keywords: Palmaris Profundus; Anatomical variation; Accessory forearm muscle; Carpal tunnel
INTRODUCTION
This case report investigates two anatomical variants of the palmaris profundus muscle found in the left and right forearms of a single cadaver. We aim to contribute to the current literature on the palmaris profundus muscle and provide a better understanding of its presence for its potential clinical and surgical implications.
The palmaris profundus (PP) muscle is a rare anatomic variant that can be found in the anterior forearm musculature. The muscle was first described by Frohse and Fränkel in 1908, and since then has been characterized as an accessory muscle generally coexisting with the palmarius longus muscle.1,2 This muscle has been found to occur in multiple variations and is characterized by its course through the carpal tunnel as it travels adjacent to the median nerve and inserts distally into the palmar aponeurosis.1
This accessory muscle has potential clinical implications such as carpal tunnel syndrome. It does this by occupying space within the carpal tunnel and potentially exerting additional compressive forces on the median nerve.3 Cadaveric studies estimate the prevalence of palmaris profundus to be less than 0.5% with one study noting its presence in 1 out of 530 cadaver limbs.1 Its presence can also cause difficulty during wrist tendon harvesting procedures. In addition, this muscle could potentially cause a compressive neuropathy of the median nerve or the anterior interosseous nerve in the distal forearm and wrist.4
CASE PRESENTATION
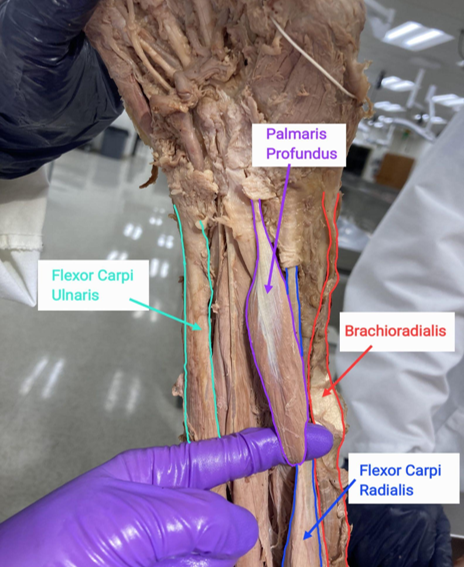
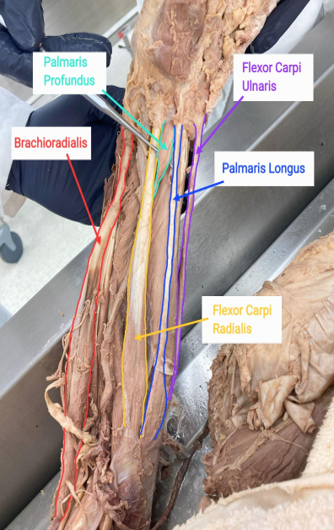
During routine cadaveric dissection at Texas A&M College of Medicine of a 97-year-old embalmed male cadaver, we identified the presence of the Palmaris Profundus muscle bilaterally. The individual had passed away from hypertensive heart disease. Typical superficial muscles of the flexor forearm were found and identified bilaterally: including the pronator teres, flexor carpi radialis, palmaris longus, and flexor carpi ulnaris. Typical deep muscles of this compartment, such as the flexor digitorum profundus, flexor pollicis, and pronator quadratus, were also present bilaterally. Two different presentations of the palmaris profundus muscle were found when comparing the right and left forearm.
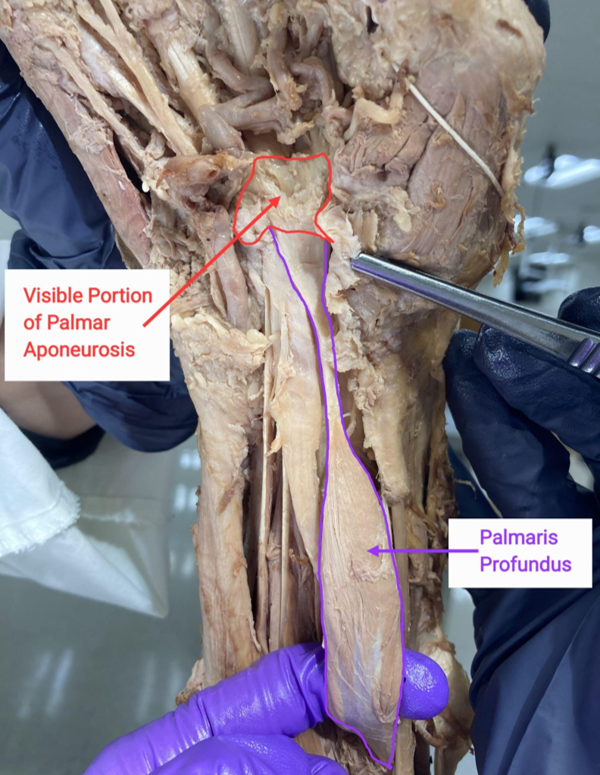
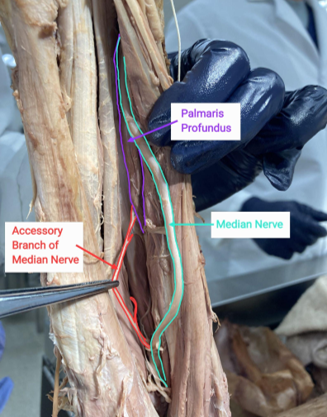
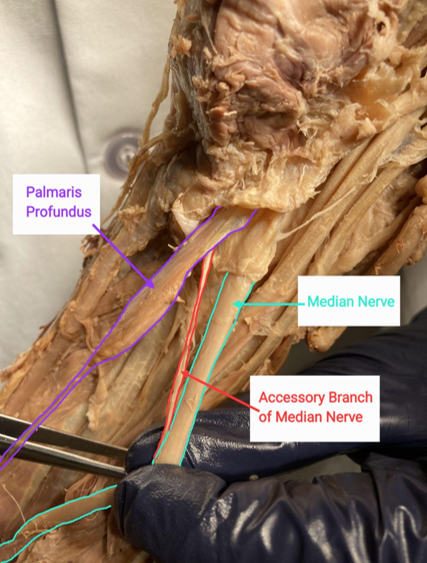
Upon further examination of the right anterior forearm, we identified an accessory muscle tendon inserting into the deep surface of the palmar aponeurosis. In this variant of the palmaris profundus, the muscle originated from the fascia of flexor digitorum superficialis and distal tendon (4.1 cm in length) traveling through the carpal tunnel and inserting deep to the palmar aponeurosis. The right palmaris profundus muscle measured 10.9 cm in height, 1.95 cm in width and 0.6 cm in thickness. The muscle displayed a fusiform belly with a proximal tendon (5.73 cm in length). The transverse carpal ligament was incised to allow visualization and confirmation of the trajectory of the distal tendon within the carpal tunnel. An accessory branch of the median nerve was found to innervate the right palmaris profundus muscle.
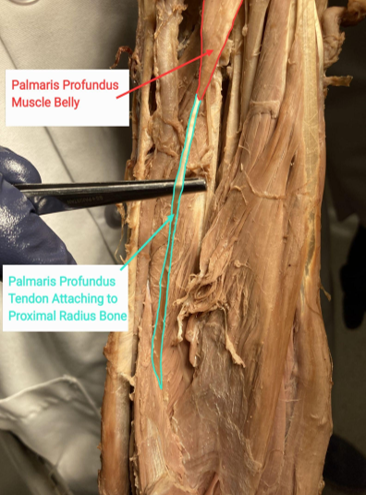
The palmaris profundus found in the left forearm demonstrated significant variance from that found in the right forearm. In this variant of the palmaris profundus on the left side, the muscle was inverted. The muscle displayed a fusiform belly originating from the deep side of the flexor retinaculum with a proximal tendon (9.55 cm in length) inserting into the humeroradial head of the radius. The left palmaris profundus muscle measured 5.45 cm in height, 1.3 cm in width and 0.5 cm in thickness. The tendons of the palmaris longus and flexor carpi radialis were transected, and the corresponding muscle bellies were reflected proximally to enhance visualization of the insertion of the palmaris profundus at the radius (Figure 4). Furthermore, blunt dissection of the radial head of the flexor digitorum superficialis confirmed the insertion of the palmaris profundus (Figure 5). An accessory branch of the median nerve was also found to innervate the left palmaris profundus muscle (Figure 6).
DISCUSSION AND CONCLUSION
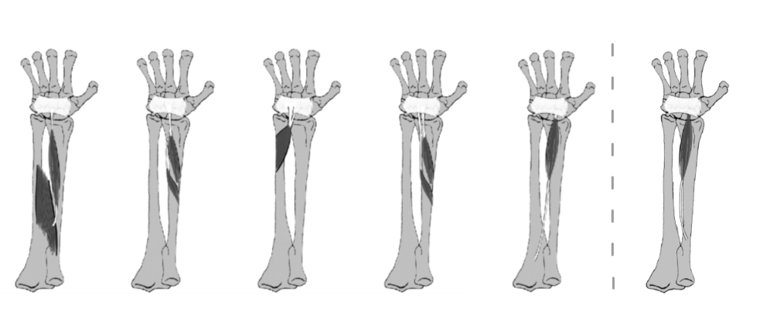
This case presents an occurrence of bilateral variations of palmaris profundus muscle. Subtypes of the Palmaris Profundus are classified based on their origin: Type 1 (A) arises from the fascia of the flexor digitorum superficialis; Type 2 (B) from the proximal or mid-third of the radius; Type 3 (C) from the anterior surface of the distal ulna; Type 4 (D) has a bicipital origin; and Type 5 (E), Palmaris profundus inversus ulnaris proximalis, originates from the proximal tendon at the ulnar shaft (See Figure 7).1,2,5 All subtypes show insertion into the dorsal side of the flexor retinaculum and the palmar aponeurosis. On the right side, a Type 1 PP (Figure 7) was identified as described in Bast et. al. This was evident as the proximal tendon originated from the fascia of the flexor digitorum superficialis and the distal tendon inserted into the deep side of the palmar aponeurosis. On the left side, we propose a previously undocumented variant of the palmaris profundus. This proposed Type VI variant, palmaris profundus inversus radialis proximalis, is similar to the Type V PP muscle due to its shared presence of an inverted muscle belly that inserts into the deep side of the palmar aponeurosis. In contrast, the Type VI PP varies with respect to its origin being the proximal tendon which connects to the proximal radial bone rather than the ulnar bone as seen in Type V PP.1,2
Palmaris profundus exhibits variable origins and insertions but is primarily characterized by its course adjacent to the median nerve through the carpal tunnel.4 It is most commonly innervated by the anterior interosseous nerve but may receive innervation from the ulnar nerve if its origin lies near the distal ulna.4 Additional variation can be present in reversed or bi-tendinous forms.
These variants can be explained through embryological planning. Embryologically, limb muscles originate from the paraxial mesoderm, which segments into somites composed of sclerotome and dermomyotome.6 All trunk and limb skeletal muscles originate from the dermomyotome, whose multipotent cells commit to specific muscle lineages in response to paracrine signaling.7 Among the key regulators of this process is MyoD, a member of the myogenic regulatory factors (MRF) family, which plays a central role in promoting myogenic differentiation.7 In the 5th week of development, myoblasts from these myotomes into these developing limbs begin to organize into muscle masses. The final patterning of muscles is regulated by specific growth signals, such as MyoD, and by programmed cell death through apoptotic signaling pathways.8 A disruption in these signalling pathways or developmental processes can result in aberrant or accessory muscle formations, such as the palmaris profundus.8
Due to cadaver desiccation, it is not possible to determine if there was any atrophy of the thenar eminence, which is a key indicator of carpal tunnel syndrome. Additionally, the handedness of the cadaver is unknown which has limited our ability to assess for asymmetry or changes related to overuse of the dominant-hand. The usual finding of larger muscles present within the dominant arm could not be determined. The absence of patient history further prevents any correlation between anatomical findings and reported symptoms of median nerve dysfunction. Lastly, postmortem tissue degradation may have masked any soft tissue or neural abnormalities which will reduce overall diagnostic clarity during our dissection.
Diagnosis in these situations can be done with patient history and physical exam findings such as positive Tinel’s and Phalen’s tests. The first line of treatment will be pain management through the use of NSAIDs if not contraindicated and splinting. Steroidal injections can be administered as a more targeted approach if prior pain management is not sufficient. Surgical carpal tunnel release will be performed as a last resort. The presence of this anatomical variation may serve as a technical challenge during endoscopic procedures. This may require the surgeon to convert a minimally invasive procedure to a more open surgical technique.9 Both surgical release of the transverse carpal ligament and excision of the distal Palmaris Profundus tendon have been shown to independently improve symptoms.
Surgeons who specialize in the hand and wrist may encounter this anatomical abnormality during procedures such as carpal tunnel release or during wrist tendon harvesting. Neurologists may also encounter this variation during the non-surgical management and treatment of carpal tunnel syndrome and anterior interosseous nerve syndrome. Additionally, anatomists and medical educators can benefit from understanding this anatomical variation. This will enhance their ability to effectively teach anatomical diversity to residents, medical students, and undergraduate students.
REFERENCES
1. Andring N, Kennedy SA, Iannuzzi NP. Anomalous Forearm Muscles and Their Clinical Relevance. Journal of Hand Surgery. 2018;43(5):455-463. doi:10.1016/j.jhsa.2018.02.028
2. Bast BO, Winkler M, Kurz B. Reversed palmaris profundus muscle variation. Int J Anat Var. 2016;9:21-24. doi:10.1007/s11552-010-9281-9
3. Riml S, Kompatscher P. Palmaris Profundus Tendon as Possible Cause for Median Nerve Compression. Journal of Hand Surgery. 2012;37(10):2198-2199. doi:10.1016/j.jhsa.2012.06.042
4. Browne KM, Fauzi Z, O’Shaughnessy M. The palmaris profundus, a rare sight during carpal tunnel release. Hand (N Y). Sep 2015;10(3):559-61. doi:10.1007/s11552-014-9691-1
5. Yoshida Y, Yasutaka S, Seki Y. [Flexor radialis profundus and palmaris profundus muscles in man]. Kaibogaku Zasshi. Apr 1983;58(2):59-67.
6. Lemos DR, Eisner C, Hopkins CI, Rossi FMV. Skeletal muscle-resident MSCs and bone formation. Bone. 2015/11/01/ 2015;80:19-23. doi:https://doi.org/10.1016/j.bone.2015.06.013
7. Endo T. Molecular mechanisms of skeletal muscle development, regeneration, and osteogenic conversion. Bone. 2015/11/01/ 2015;80:2-13. doi:https://doi.org/10.1016/j.bone.2015.02.028
8. Saravanan K, Kumar R, Borthakur D, Kusuma H, Singh S. Accessory Flexor Muscle of Forearm – A Rare Variant – Embryological and Clinical Prospect. Prague Med Rep. 2024;125(4):356-364. doi:10.14712/23362936.2024.32
9. McClelland WB, Jr., Means KR, Jr. Palmaris Profundus Tendon Prohibiting Endoscopic Carpal Tunnel Release: Case Report. Journal of Hand Surgery. 2012;37(4):695-698. doi:10.1016/j.jhsa.2012.01.006